



Carpal tunnel syndrome (CTS) causes a tingling sensation, numbness and sometimes pain in the hand and fingers. Tim McClure takes a look at this common, but often restrictive, disorder.
Musculoskeletal disorders are defined as injuries and disorders affecting the body’s musculoskeletal system – this includes the joints, muscles, tendons, ligaments, nerves and discs.1 There are over 100 different types of musculoskeletal disorders, ranging from the very common to the extremely rare.2 These disorders can be episodic or chronic in duration and may progress in their severity over time. Though seldom life threatening, musculoskeletal disorders impair the quality of life of a large proportion of the adult population.3
Carpal tunnel syndrome (CTS) is a common musculoskeletal disorder that can affect the activities of daily life and sleep. It is the most common compression neuropathy of the upper limbs. With most studies citing prevalence at around five per cent in the general population and incidence on the increase, community pharmacists are ideally placed to counsel those affected with CTS in the primary care setting.4
Causes
The carpal tunnel comprises eight small carpal bones, bound by the carpal ligament that lies across the palm-side of the wrist. Between this ligament and the carpal bones forms a passage called the carpal tunnel, through which various tendons and the median nerve pass. The median nerve gives feeling to the thumb, index and middle fingers and half of the ring finger, in addition to controlling movement of small muscles at the base of the thumb.5 Anything that decreases the amount of space in the carpal tunnel, or increases the pressure within it can compress the median nerve and potentially lead to symptoms of CTS.6,7 In most cases, the cause of CTS is not known.8 However, there are certain recognised risk factors. These include:
- Activities with high hand/wrist repetition rate
- Pregnancy (up to 50 per cent of pregnant women develop CTS)
- Obesity
- Injuries to the wrist including fractures
- Patients with rheumatoid arthritis
- Family history of CTS (about one in four people with CTS have a close family member who also has or had the condition)4,5,7,8
CTS is three times more common is women than men, and becomes more likely as you get older.8 Studies have shown strong evidence to support the increased risk of CTS associated with overuse of the hand and wrist in such jobs as assembly line work, gardening and occupations requiring a forceful grip. There is less robust evidence to suggest an association between computer-based work and CTS.7 Interestingly, some studies show that CTS is actually less common in people who type all day than in those who carry out more strenuous activities.8
Symptoms
CTS encompasses a collection of symptoms including intermittent tingling, altered sensation, pain, weakness and impaired fine manipulation.7
Paraesthesia (pins and needles) is typically the first symptom to develop. This sensory loss is within the distribution area of the affected median nerve (see diagram 1). This area consists of the thumb, index and middle finger and half of the ring finger. Pain in the same area may then present and can radiate up the arm into the wrist or as far as the shoulder. Numbness in the hand, wrist or forearm can develop if the condition progresses. Symptoms tend to worsen when the hand or wrist is in action, for example when gripping an object or flexing the wrist.5,6,7 In severe cases, weakness of some muscles in the fingers and/or thumb can occur. This may cause poor grip and eventually lead to muscle atrophy and reduced strength at the base of the thumb. The skin around the thumb, index and middle fingers can also become dry.7
Symptoms often occur in both hands, but they are usually worse in one hand than the other. Most cases affect both hands eventually. Typically, CTS sensations present intermittently to begin with and develop gradually over time with most noticing their first symptoms occur at night – this can cause the sufferer to awaken.6 CTS can lead to difficulties with daily activities, including work, and sleep. It is therefore a recognised cause of reduced productivity in the workplace.7 If the condition becomes severe, symptoms can persist all day.6
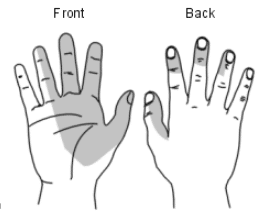
Diagram 1 – CTS symptom distribution.
Shaded areas show where symptoms typically occur.5
Diagnosis
Symptom presentation alone is often enough for a positive CTS diagnosis. Although not a stand-alone test to diagnose CTS, a positive Phalen’s test can help in the identification of this musculoskeletal disorder. Phalen’s test is positive if flexing the wrist for 60 seconds causes pain and paraesthesia in the median nerve distribution area (ie, thumb, index and middle fingers and half of the ring finger). Blood tests or nerve conduction studies are reserved for where there is diagnostic doubt, in complex cases or where examination suggests a specific secondary casue.7
Treatment options
In up to one in four cases of CTS, symptoms resolve without treatment within one year. With regards to those cases of CTS that develop during pregnancy, symptoms disappear in about two out of three cases three months postpartum.5,8 Symptoms are most likely to spontaneously resolve in people aged under 30, those with pregnancy-related CTS, persons with only unilateral involvement and those with a negative Phalen’s test.5,7
The goal of treatment for CTS is to restore the patient’s normal functions and activities in addition to preventing nerve damage and loss of muscle strength in the fingers and hand. Treatment options are generally divided into three main categories: home treatment, medication and surgery.6
Home treatment – If CTS is mild, two to four weeks of home treatment is likely to relieve symptoms. The aim here is to ease pain and prevent further or permanent damage to the median nerve. Symptoms can be completely relieved if treatment is started when symptoms first occur.6,8 Strong evidence supports immobilisation of the wrist with the use of a removable wrist splint.7 The aim of the splint is to maintain the wrist at a neutral angle without applying any force over the carpel tunnel. Splints are designed to hold the wrist in the position where the carpal tunnel pressure is lowest, ultimately relieving pressure on the median nerve. The stiff metal support which gives these devices rigidity should be bent specifically to fit the patient’s wrist and should be arched over the carpal tunnel area itself so that it doesn’t apply direct pressure to the median nerve from the outside. Splints should be worn whenever they do not obstruct activities. In particular, they are helpful with night-time symptoms, with use of the device at night alone often sufficient to provide relief after a few weeks of use.6,8
Icing the wrist for ten or fifteen minutes at intervals during the day can temporarily help to relieve pain.6 Lifestyle modifications such as the use of ergonomic equipment like wrist rests, taking breaks from repetitive tasks and alternating job functions are all traditionally advocated in the management of CTS, but the evidence supporting their effectiveness is inconsistent.8 At the very least, patients can be advised to rest the fingers, hand and wrist whilst stopping activities that cause numbness and pain. When symptoms have improved activities can gradually be resumed, with wrists kept straight or only slightly bent.6
Medication – Although theoretically reducing inflammation in the carpal tunnel, there is little evidence to support the use of non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen to treat CTS. NICE guidelines state that NSAIDS should not be recommended. Additionally, doctors should not prescribe diuretics as part of a treatment plan for this condition.7,8
There is strong evidence to support the administration of a corticosteroid injection into the wrist for chronic CTS.7 This measure should only be considered after conservative treatment such as rest, ice and splints have been tired for several weeks with no improvement. Corticosteroid injections often provide temporary relief lasting several weeks or more, but rarely provide permanent relief from carpel tunnel symptoms.6
There is no evidence to support the use of complementary medicine such as acupuncture or dietary supplements like pyridoxine in the management of CTS. 6
Surgery – Only a minority of patients with CTS are treated with surgery. This form of treatment is only considered in specific circumstances. For example:
- If symptoms have not improved after several months of non-surgical treatment, assuming there is no nerve damage
- If nerve test results show damage to the median nerve
- If symptoms are extreme enough to restrict normal daily activities due to persistent loss of feeling, reduced thumb strength or if sleep is severely disturbed
The most common CTS surgery involves cutting the carpal ligament to reduce pressure on the median nerve in the wrist. This is performed under local anaesthetic. The procedure can either be carried out as open or endoscopic surgery. Open carpal tunnel release surgery requires a longer recovery period and leaves a large scar, but there is less incidence of complications. Conversely, endoscopic carpal tunnel release surgery is quicker and leaves a smaller scar, but there is a small increased chance of requiring further surgery. There are no long-term differences in the outcomes of these two approaches.6,8